By Cassandra Biro, Debbie Luk
What is Myopia and how do you correct it?
Myopia (near-sightedness) results when the power of the cornea is stronger and/or the length of the eye is longer than average. This results in light focusing in front (instead of on) the retina making distant objects appear blurry and near objects appear clear. Myopia is corrected with minus lenses which diverge light onto the retina.
How common in Myopia and when does it develop?
The prevalence of myopia varies significantly by geographic location. It is more common in Asian and Hispanic children relative to Blacks and Caucasians. It usually progresses at half a diopter per year starting roughly around the age of 8 until about 16 years old. Although there is no single gene tied to its development, studies have shown that the more myopic parents one has the higher their chances are of developing it.
Why is myopia control important?
High myopia (> -6.00 D) increases one’s chances of developing sight-threatening conditions such as retinal detachments, glaucoma, and cataracts. Furthermore, spectacles for these prescriptions are not only more expensive but also appear thicker compared to standard lenses.
What Causes Myopia Progression?
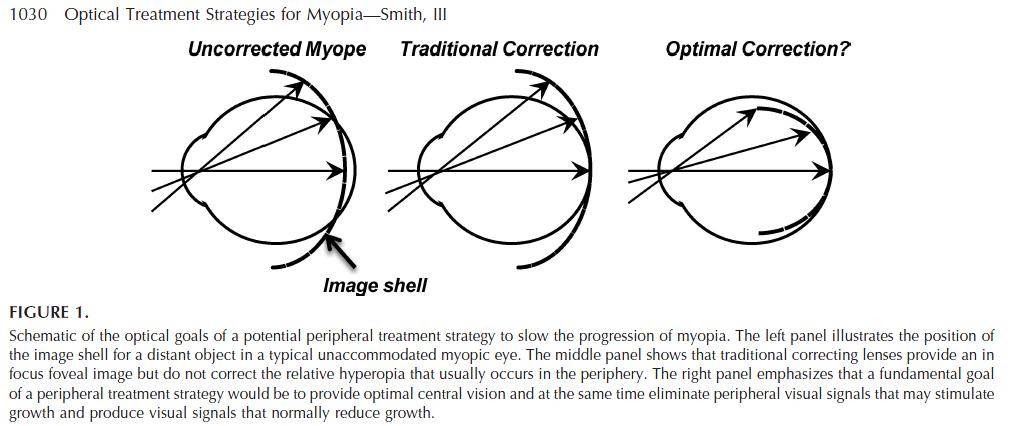
The exact cause of myopia progression is unknown. One theory suggests that myopes have peripheral hyperopia which worsens with correction. This means that although light travelling through the center of the spectacle lens is formed on the retina, the peripheral rays focus behind the retina which stimulates the release of neurotransmitters (likely dopamine) causing the eye to elongate. Other mechanisms implicated in the progression of myopia include accommodative lag (the image forms behind the retina due to inability to provide enough focus at near) and near esophoria (inward resting position of the eyes at near which leads to too much focusing for a given target and an image that lies in front of the retina).
How is myopia control carried out?
Various methods have been suggested for myopia control however, the most effective approaches based on current research are orthokeratology contact lenses, soft bifocal contact lenses, and Atropine eye drops. Orthokeratology involves the use of hard contact lenses to reshape the cornea overnight. These lenses are only worn while sleeping where the lid applies pressure to the lens leading to flattening of the central cornea and steepening of the periphery. This method corrects the central myopia by putting the image onto the retina and leaves the peripheral rays focused in front of the retina instead of behind. The advantage of orthokeratology is that once the lenses have been worn consistently, the individual will not have to wear correction during the day. Disadvantages include a risk of bacterial infection due to overnight wear as well as cost. Soft bifocal contact lenses are worn during the day and work in a similar manner to orthokeratology lenses in that their design allows for central rays of light to be focused on the retina while leaving peripheral rays focused in front. Cost of these lenses varies with the brand and modality (e.g. dailies, bi-weeklies, monthlies) nonetheless they are generally well tolerated and there is a lower risk of bacterial infection with daily wear. Finally, instillation of 0.01% Atropine eye drops once daily (for a minimum of two years) has shown to be effective in preventing progression of myopia in 6-12 year olds with marginal side effects. The exact mechanism of this anti-muscarinic drug is unknown however, it may be a more economical option as well as an alternative for those children who cannot tolerate contact lenses.
Will more time outdoors help with controlling my child’s myopia?
Studies have shown that outdoor activity does not provide an effective method of controlling myopic progression however, it may help to prevent the onset of myopia in children. Taiwanese researchers have found a higher incidence of myopia in children that maintained their regular recess routine (18%) compared to those that were encouraged to play outside (8%).
Are these methods FDA approved?
At this time, all of these approaches to myopia control are not FDA approved due to their novelty. Usage is considered off-label however with proper counselling from an optometrist and patient consent they can be carried out.
Works Cited:
Chia, A., Lu, Q., & Tan, D. (2016). Five-Year Clinical Trial on Atropine for the Treatment of Myopia 2. American Academy of Ophthalmology, 123(2), 391-399.
Jeffrey, W. J. (2016). Myopia Control: A Review. Eye & Contact Lens, 42(1), 3-8.
Nagra, M., & Logan, N. (2016). Myopia control-intervention strategies. Johnson and Johnson Vision Care, 46-50.
Smith, M., & Walline, J. (2015). Controlling myopia progression in children and adolescents. Adolescent Health, Medicine and Therapeutics, 6, 133-140.
Wu PC, Tsai CL, Wu HL, Yang YH, Kuo HK. Outdoor activity during class recess reduces myopia onset and progression in school children. Ophthalmology. 2013;120(5):1080–1085.
